Improving cardiovascular health in areas of inequality through early detection as a means of prevention.
Introduction:
Cardiovascular disease or CVD is a general term for conditions that affect the heart and blood vessels. It is the leading global cause of death - three-quarters of these deaths occur in countries of low and middle socioeconomic status. In England alone, people living in areas of ‘deprivation are four times more likely to die prematurely.
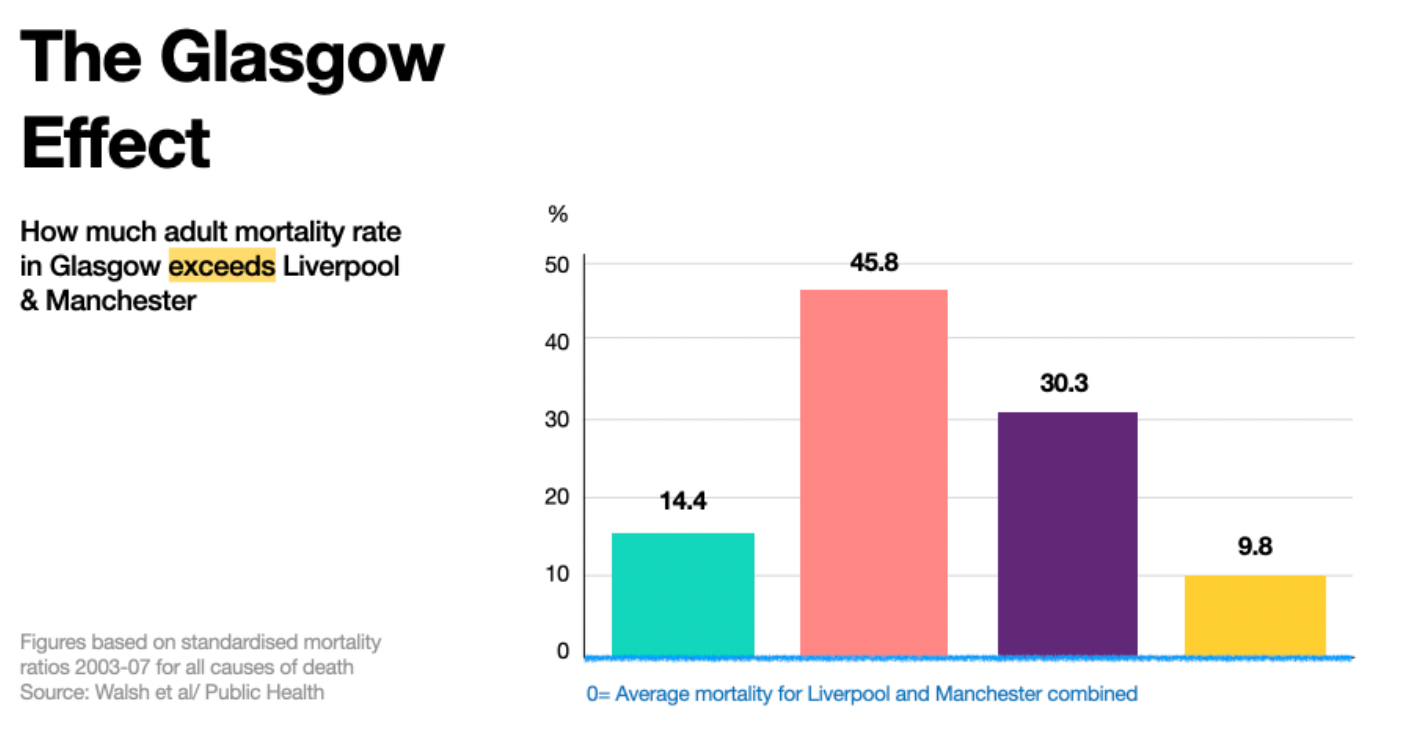
The Glasgow Effect
At the beginning of the 20th century, Glasgow had one of the highest population densities in the world, some areas being considered the worst slums in Britain. Even today, Glasgow deals with high levels of socio-economic deprivation (homelessness and housing instability, economic and employment insecurities), along with high rates of smoking, drug, and alcohol use. Glaswegians have a 30% higher risk of dying before they are 65. This excessively high mortality rate in Glasgow has been coined, “The Glasgow Effect”.
What does the Glasgow Effect have to do with cardiovascular disease?
CVD risk factors are the same health determinants contributing to the Glasgow Effect. Primary risk factors of CVD are poor diet, lack of physical activity and obesity, smoking, alcohol use, poor air quality, and high blood pressure.

Risk Factors of CVDs
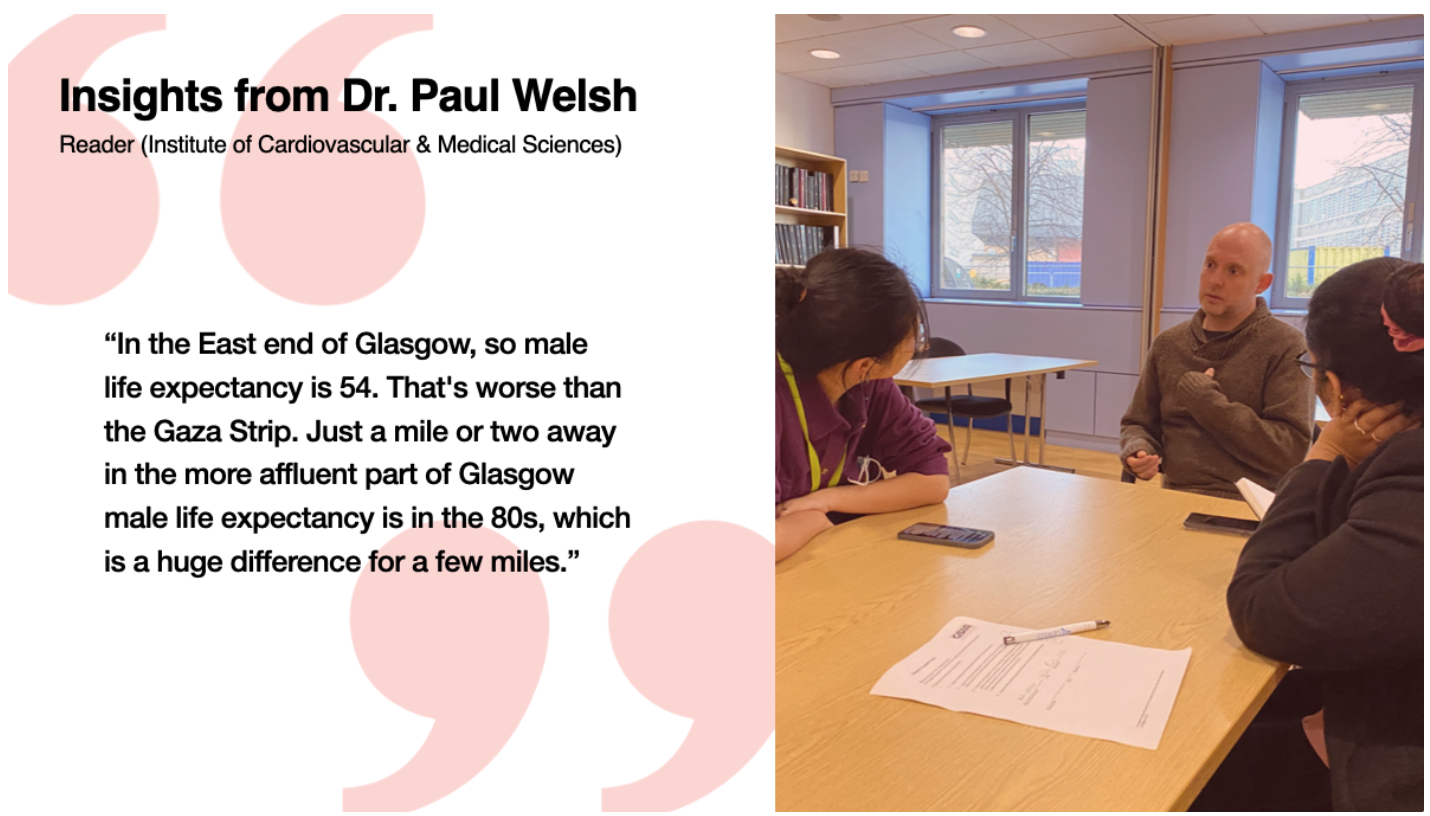
To further explore the relationship between Glasgow and CVD, we met with Dr Paul Welsh, a professor of cardiovascular and medical sciences at the University of Glasgow.
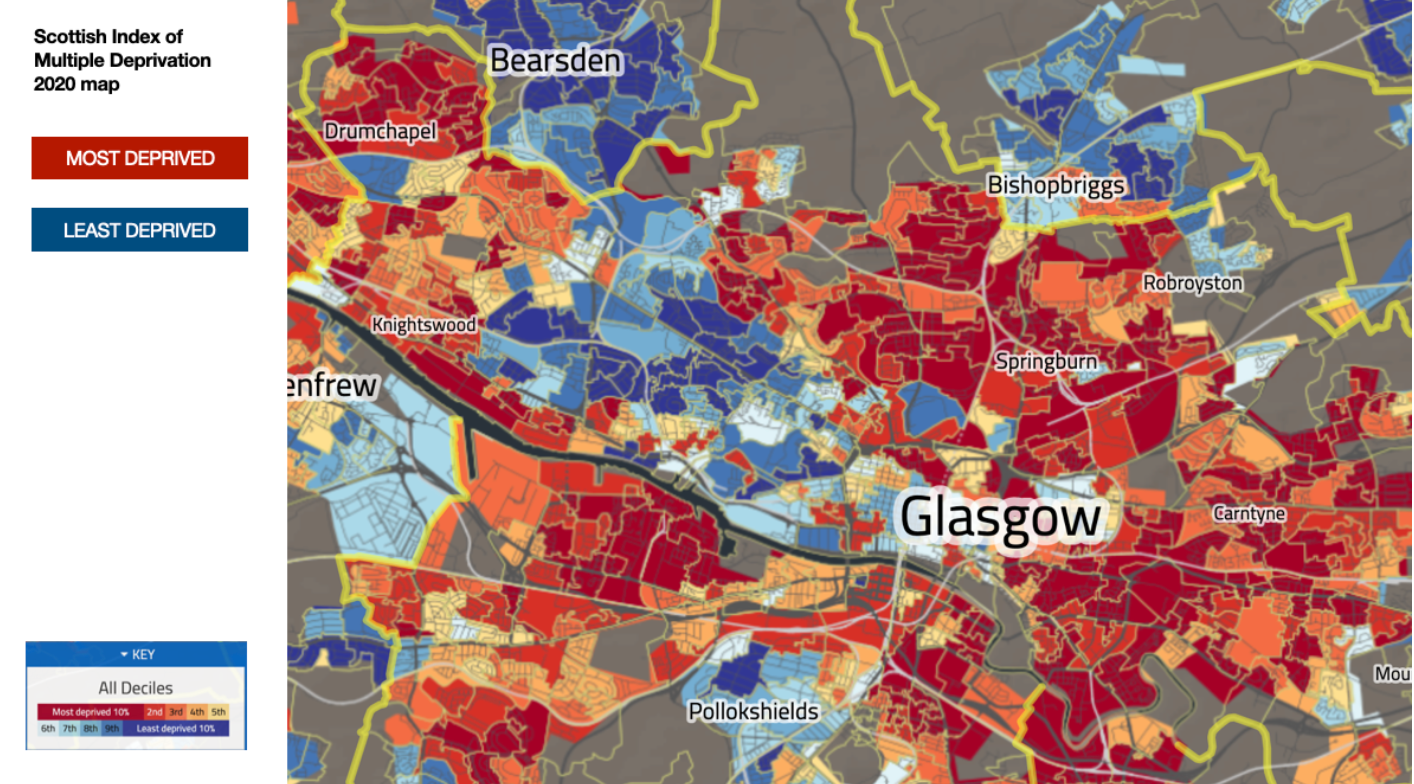
As a result of this interview and our desk research, we came to the conclusion that because people of low socio-’economic status already face enough barriers, our solution should not place the ‘onus on the individual. Rather the problem is a systemic issue that requires a preventative approach. A BBC article published in 2020 names Carntyne West and Haghill as two of the most deprived neighbourhoods in Glasgow, according to the Scottish Index of multiple deprivations. This directed us to focus on the east end of Glasgow. From here we developed a challenge statement for the project: Our intervention is early detection as a form of prevention.

We learned the impacts covid has had on children’s lifestyles; the relationship between Brexit and GP shortages; of developments in at-home testing methods; public health campaigns targeted at heart health; and how poor communities struggle to access appropriate health care.
The Problem Identified:
A systemic issue that requires a preventative approach
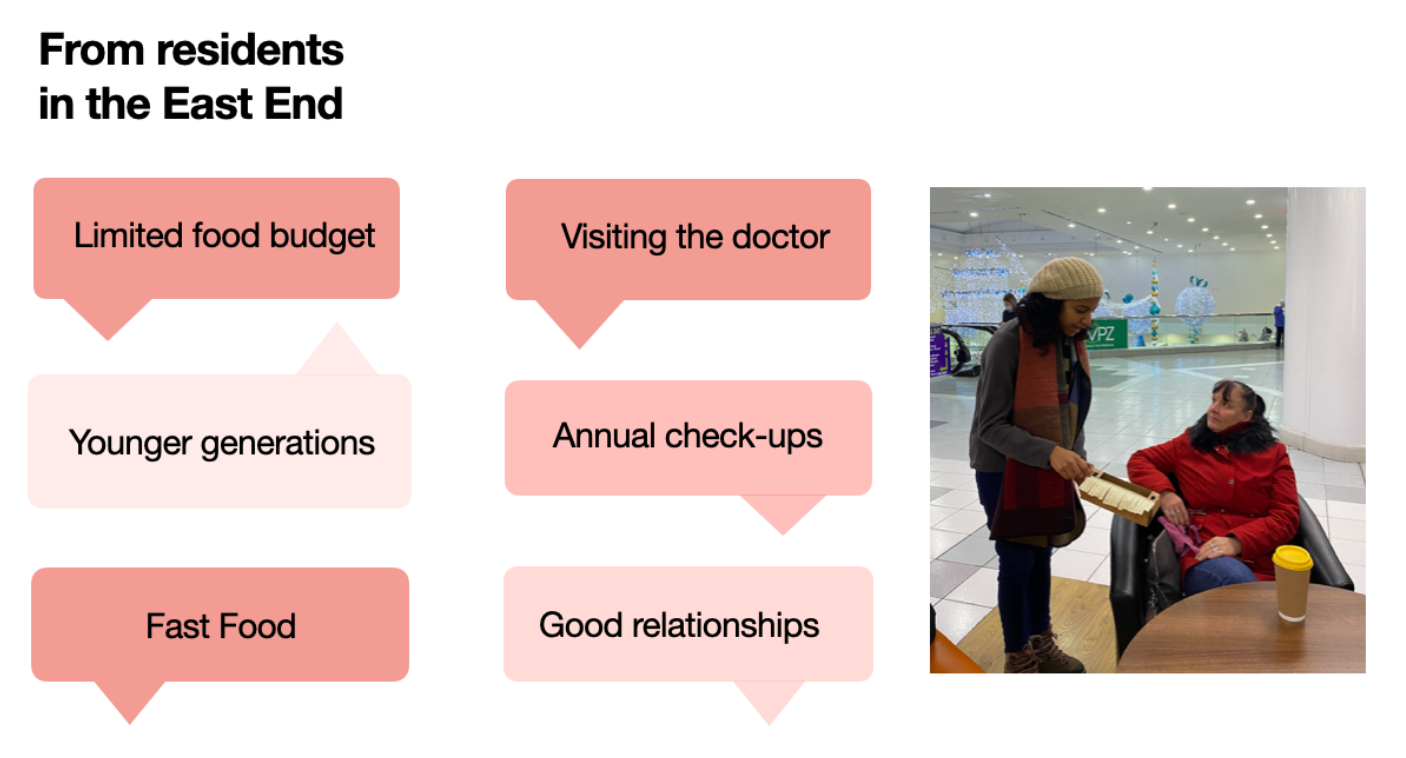
We went to the east end to interview residents and gather supplementary data through engagement tools. The residents we spoke with have lived in the area for many years and have a good relationship with their GP, but do not agree with how seldom the NHS ‘recommends check-ups.
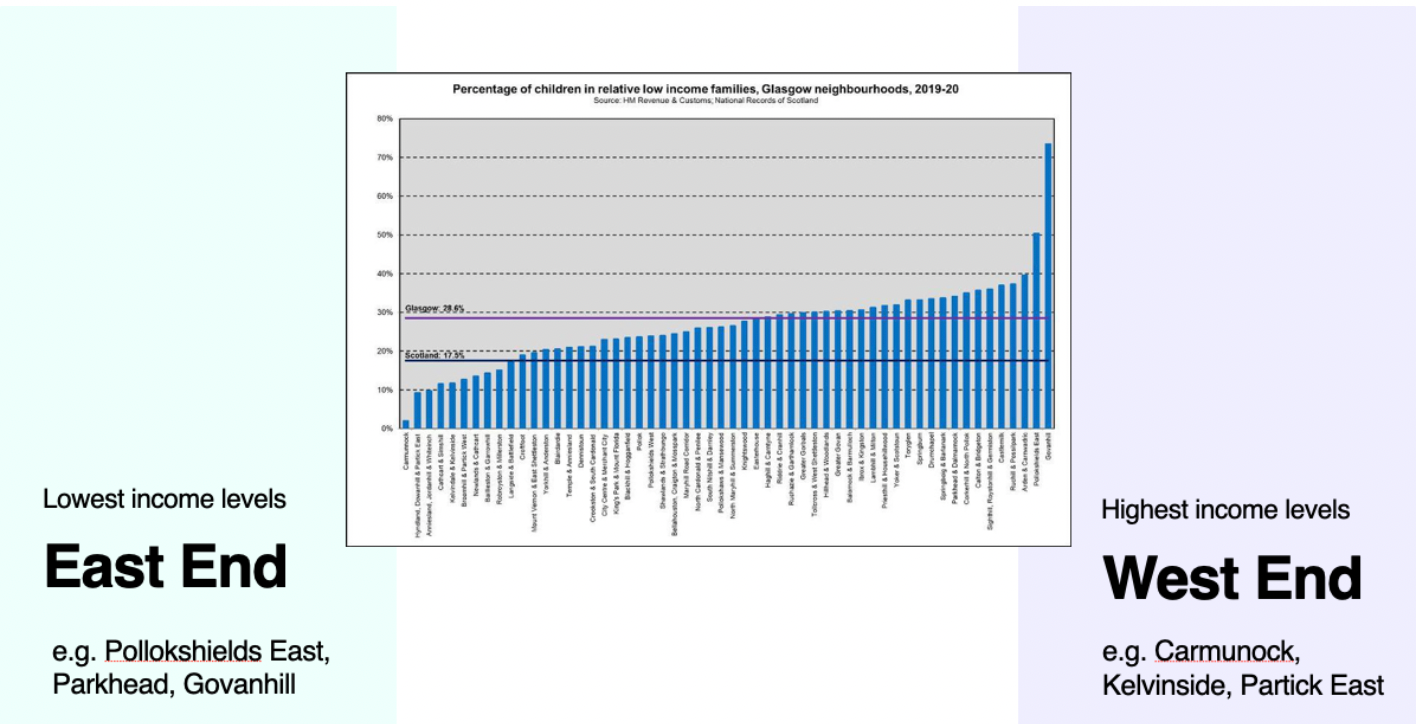
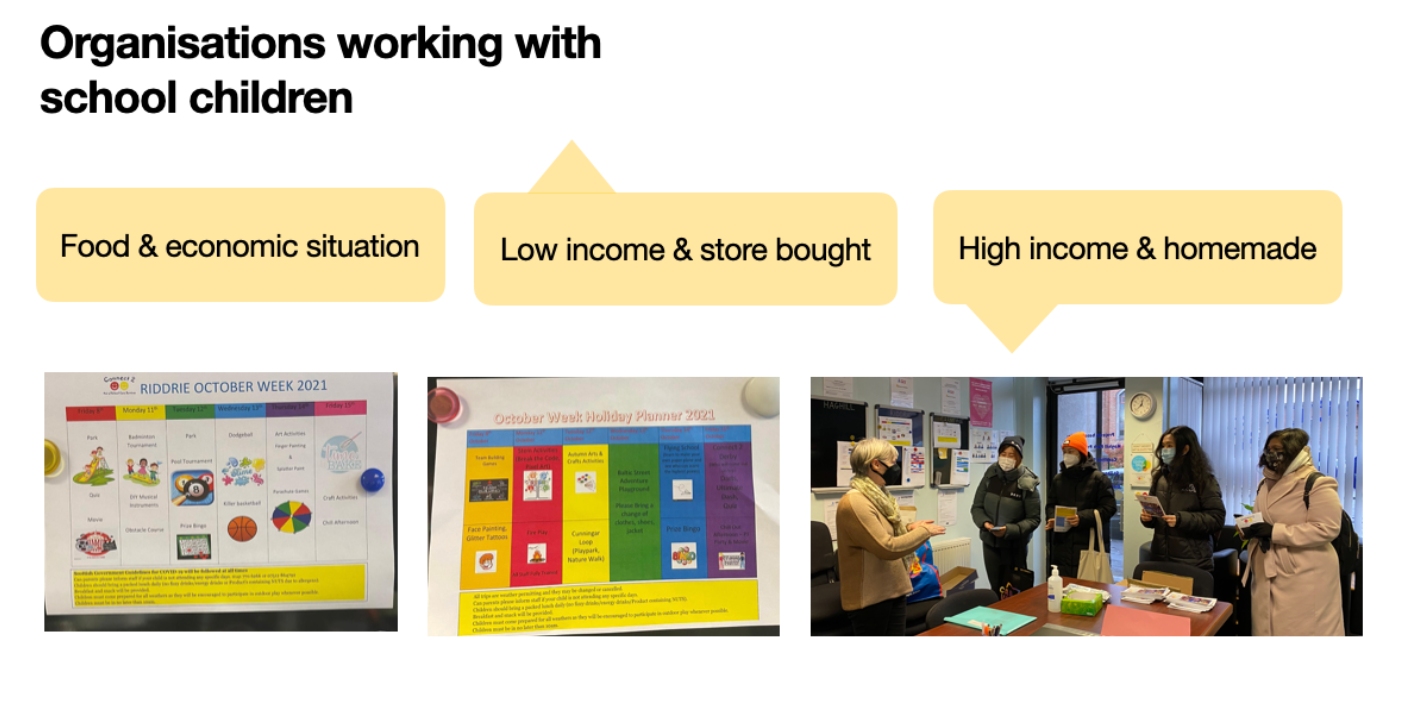
At an out-of-school child care centre, staff noted how children of low-income families generally bring pre-packed food instead of homemade meals. These families may not have access to or an understanding of healthy food.
Proposed Solution:
Early Detection as a form of Prevention.
Why Primary School Children?
Our visit to the east end exposed gaps in the current health and education systems. Patients have a strong relationship with their doctors but do not see them enough, and school children are being exposed to risk factors their care providers may not be aware of.
Currently, the child health surveillance program exists in schools as a means of tracking the general health of at-risk children when requested by a care provider. This program is not a continual assessment and is limited in its scope. It is done in isolation from the NHS system without a direct communication link.
How might we improve cardiovascular health and address these health inequalities?
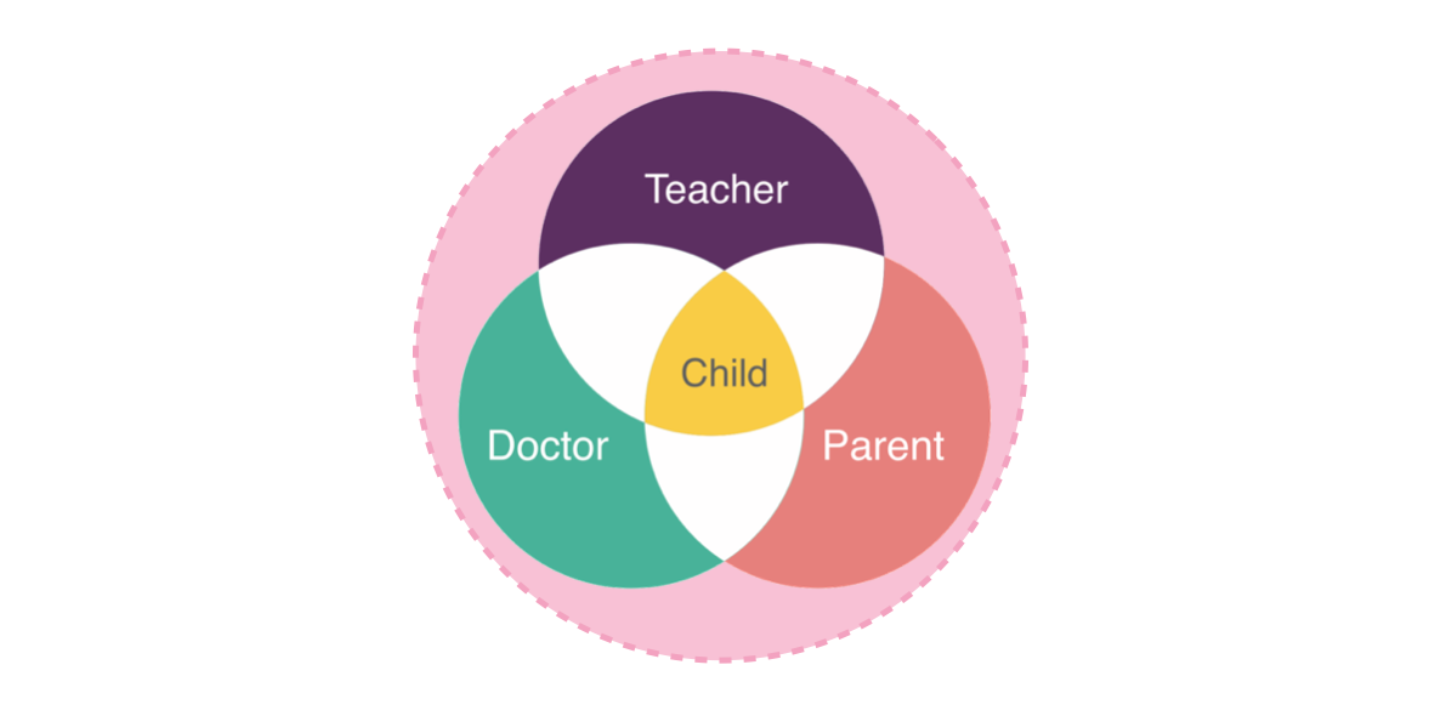
As it stands, communication regarding the child exists between the teacher and parent, and the parent and GP. To complete this communication circle, we are creating a channel for GPs and teachers to connect.
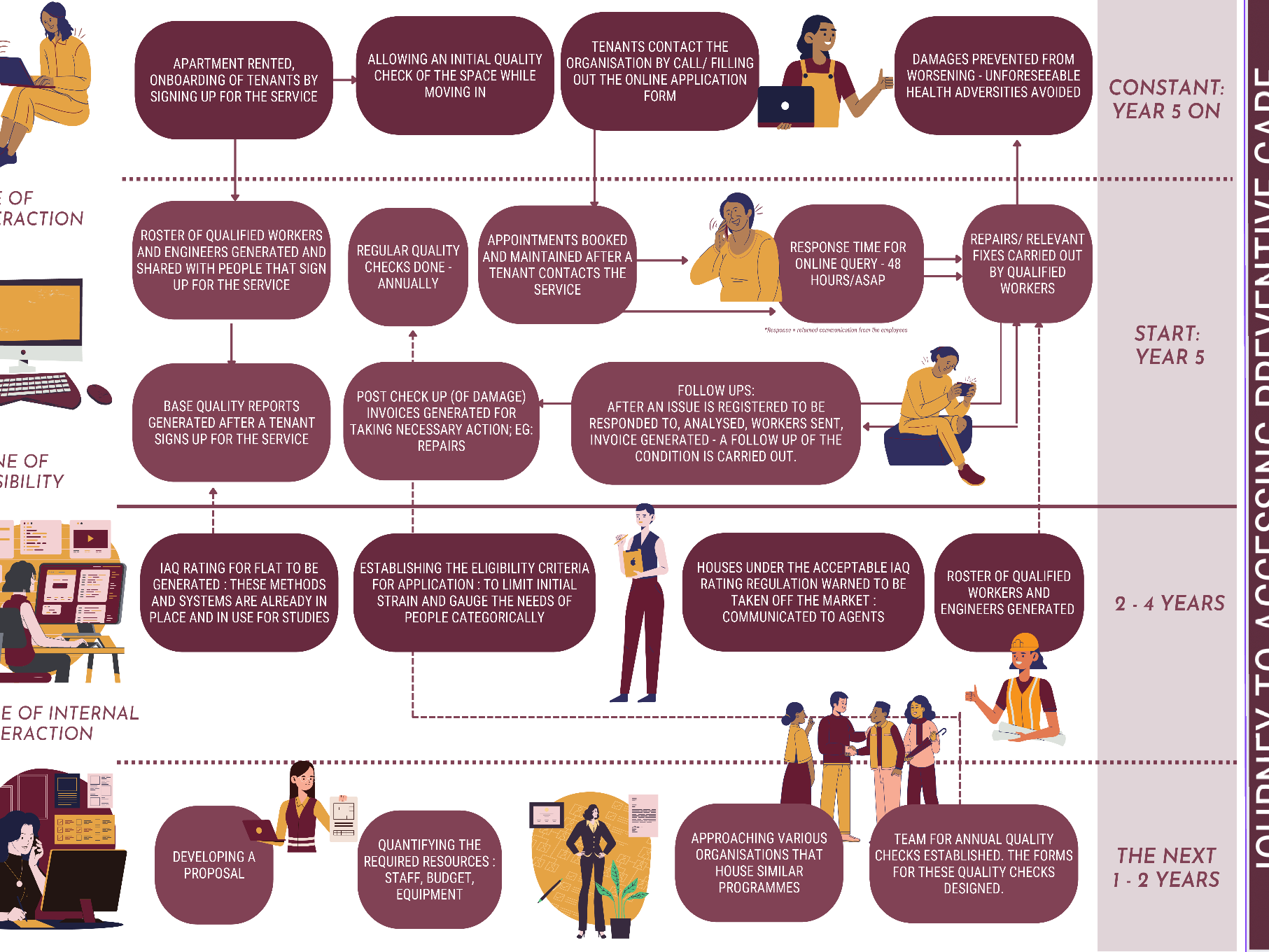
Our intervention is a program integrated into the primary school and NHS system. The central premise of this program is based on the child health surveillance program. General health observations and medical data are gathered over time, by teachers and GPs to make more appropriate care decisions.
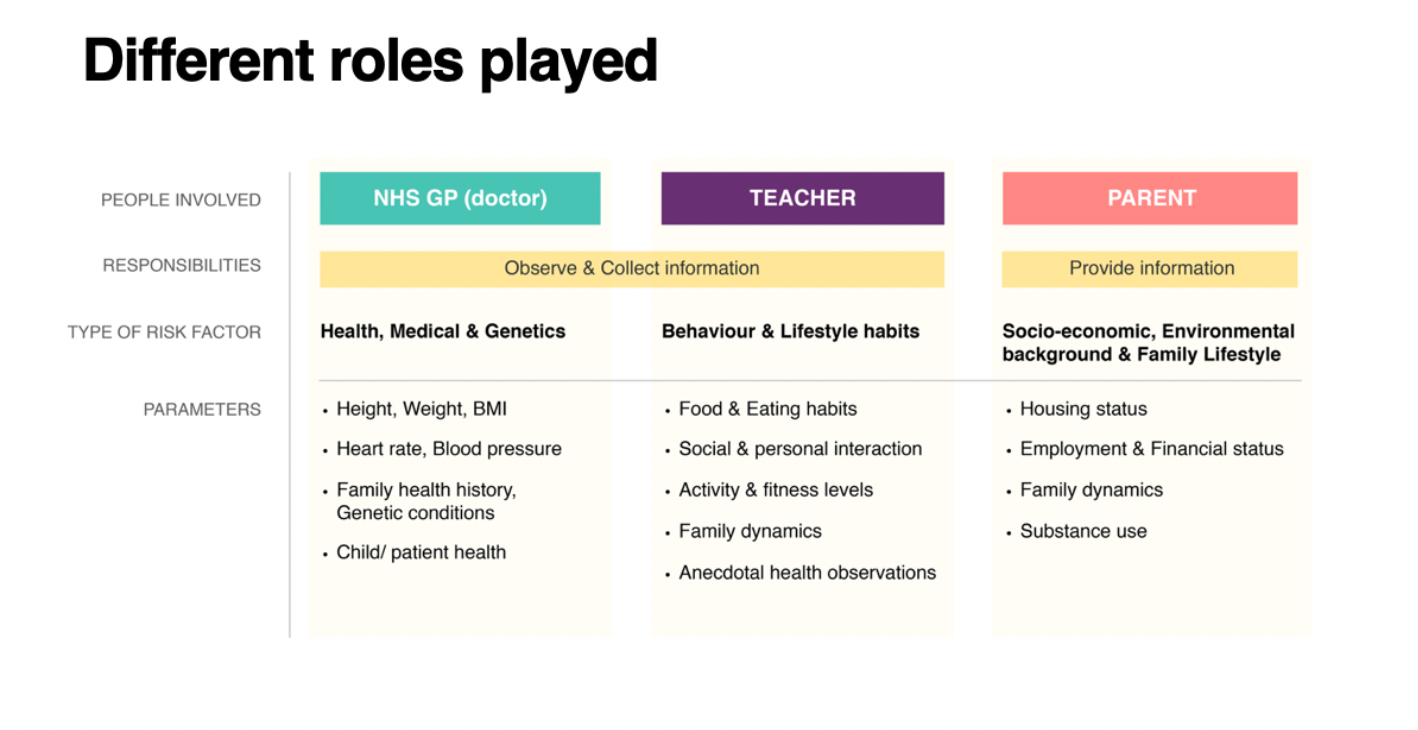
To further explain how this program functions, let’s explore the roles of care providers: the GP, teacher and parent. In terms of collecting medical information, the role of the GP remains the same.
It is the teacher who spends most of the day with the child, observing their growth and development. Their role in this program is to monitor more specific behavioural habits and the lifestyle of the child.
The parent is responsible for providing as much accurate information as possible to the GP and teacher, regarding their socio-economic position, family situation and health history.
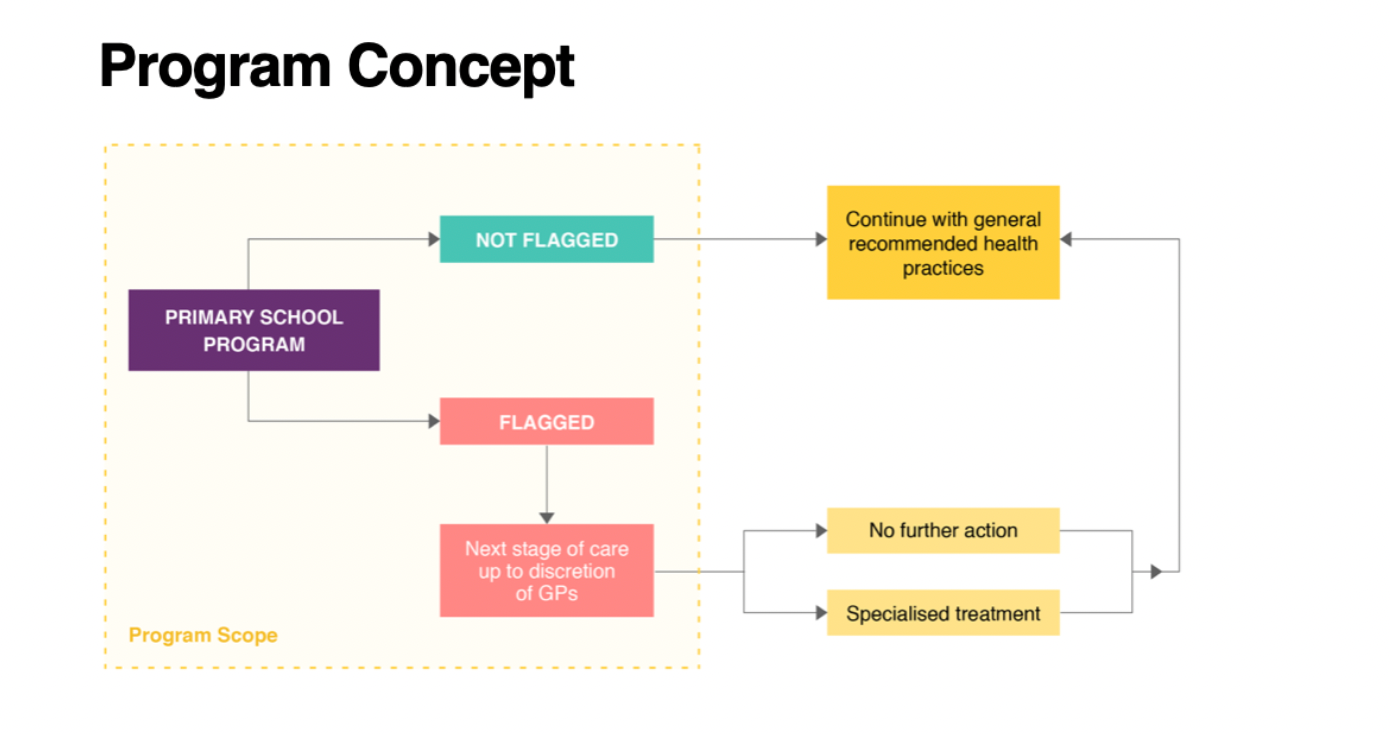
Flagging:
Communication between the GP and teacher is primarily through the concept of flagging. When a teacher notes the child meets the criteria for a risk factor, flagging happens and the GP is notified. For this to work, the teacher’s observations are added to the child’s NHS profile.
The teacher is not responsible for making any health care decisions, this is left to the GP.
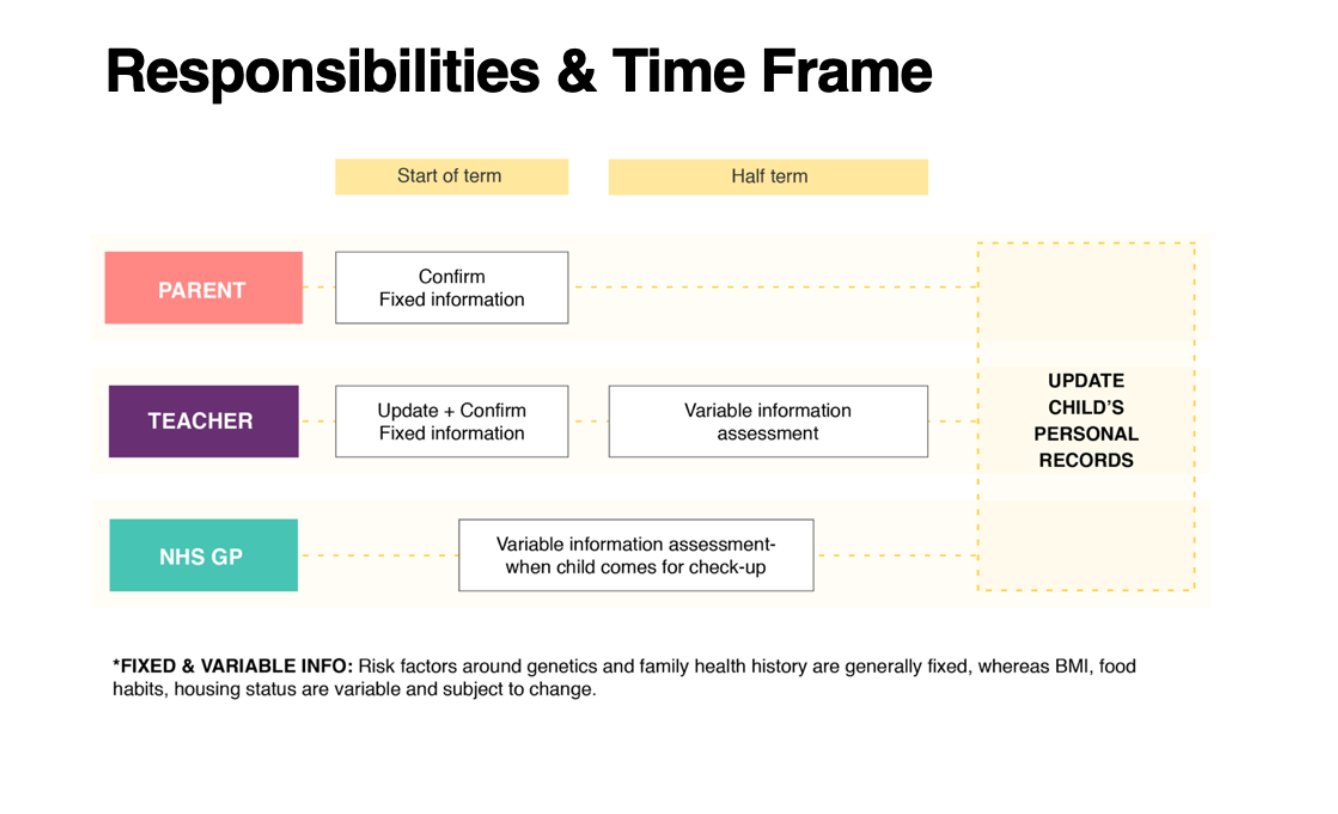
Timeline:
At the term start the teacher and parent update or confirm fixed information. Fixed information can be addressed and contact information.
At half-term, the teacher reviews variable information based on their observations.
At some point during the year, the child may have to see their GP. Variable and fixed information has been added to the child’s NHS profile.
Future Scope and Scalability
Preventative care does not begin and end in primary school. We hope that this program would be integrated into all levels of school across Glasgow, eventually further involving the child. Ideally, this routine of tracking their health becomes more normalised and integrated into their adult life.
We recognise that not all parents may wish to partake in this program. While this may prevent the child from being flagged earlier for cardiovascular disease risks, opting out is always available if requested.
How will our programme improve the lives of those with CVDs?
We hope that our program will improve the lives of those with CVD. Our goal aligns with three of the UN sustainable development goals, #1 No poverty, #3, Good health and well-being, and #10 reduced inequalities.
Focusing on the east end of the city, we hope to tackle Glasgow’s low life expectancy by recognizing CVD risk factors. Areas of poverty as a result of historically poor living conditions may contribute to higher levels of cardiovascular disease.
Tracking primary school students through general health and well-being data, this program is an early intervention to encourage preventative care measures, hopefully improving the quality of life for all its participants. This applies to everyone of all ages. We can reduce inequalities by improving access to health care. By taking the onus off the individual, we acknowledge the barriers they may face in regard to health and care decisions. This program does not have any financial expectations from its participants.
Expected challenges:
While we hope the implementation and outcomes of this project will be successful, we acknowledge there may also be challenges. Primarily, the budget and administration required to build this program could be costly. Syncing systems between the NHS and school systems could be complex with a steep learning curve.
Finally, there is the challenge of students and their guardians. This program requires that parents divulge sensitive information about their socio-economic situation. If a guardian wishes to opt-out, the child will not be tracked and could be unknowingly at an increased risk for CVD.
If a child does not attend school regularly or does not attend in the first place, it will be difficult to track and monitor their health. At the end of the day, it is not only the changes that parents and children wish to make but the responsibility that doctors have for the health and wellbeing of their patients.
This project was done in collaboration with Lena Wood, Anushree Chokappa, Kano Hashida, Yi Han, Yucong Zhu